Winter is coming: How much would it cost to keep the pressure down?
15 November 2017
The evenings are drawing in, and NHS minds are once again focusing on the impending winter pressures.
Over the last few years, even the best run hospitals have faced increasing problems achieving the national target to treat people within 4 hours of arriving at A&E. The number of people attending A&E has continued to grow, as has the proportion admitted as an emergency. But as funding fails to keep pace with demand, the prospect of hitting the 4-hour target seems to slip further away every year. Hospitals are now struggling to meet the target all year round, leading the Chief Executive of the NHS Confederation to say ‘the winter crisis is now an all year round crisis’.
The government’s ambition extends beyond just getting through this winter. Its annual mandate to the NHS sets an expectation that overall 95% of people will be seen within 4 hours by March 2018, in accordance with the national target. In previous years, a winter relief fund was set up to help manage seasonal pressures, before being incorporated into CCG budgets in 2015/16.
Of late, there have been substantial efforts to prepare for this winter. Recent measures taken to help reduce pressures include an increase in people having the flu vaccine, more 111 calls being handled by clinicians and £100m of capital investment.
However the true impact of these measures is not yet known, and there have been calls for additional dedicated funding to help providers improve access to emergency care for patients. But how much would it cost to meet the 95% target this winter? And if the money was available, is it already too late?
We estimate it would cost at least an extra £360m to add sufficient capacity to meet the national 4-hour standard for A&E this winter. But it may already be too late to wisely invest this in the most effective way.
With the help of three charts, here is how we’ve worked this out:
- Firstly, we need to look at how many people are likely to attend A&E this winter.
- Secondly, how many of those are likely to wait longer than 4 hours.
- Then, how many of these are severe enough to require an emergency admission to hospital?
In each case, the trends follow a clear seasonal pattern, which we’ve accounted for to produce projections for the likely activity exceeding the 4-hour target between January and March 2018. (Note: these are projections, not predictions. The true value will be affected by many factors including the weather or severity of any outbreak of flu.)
Finally, we then need to estimate the extra capacity that would be needed in A&E and inpatient departments to get back up to 95%.
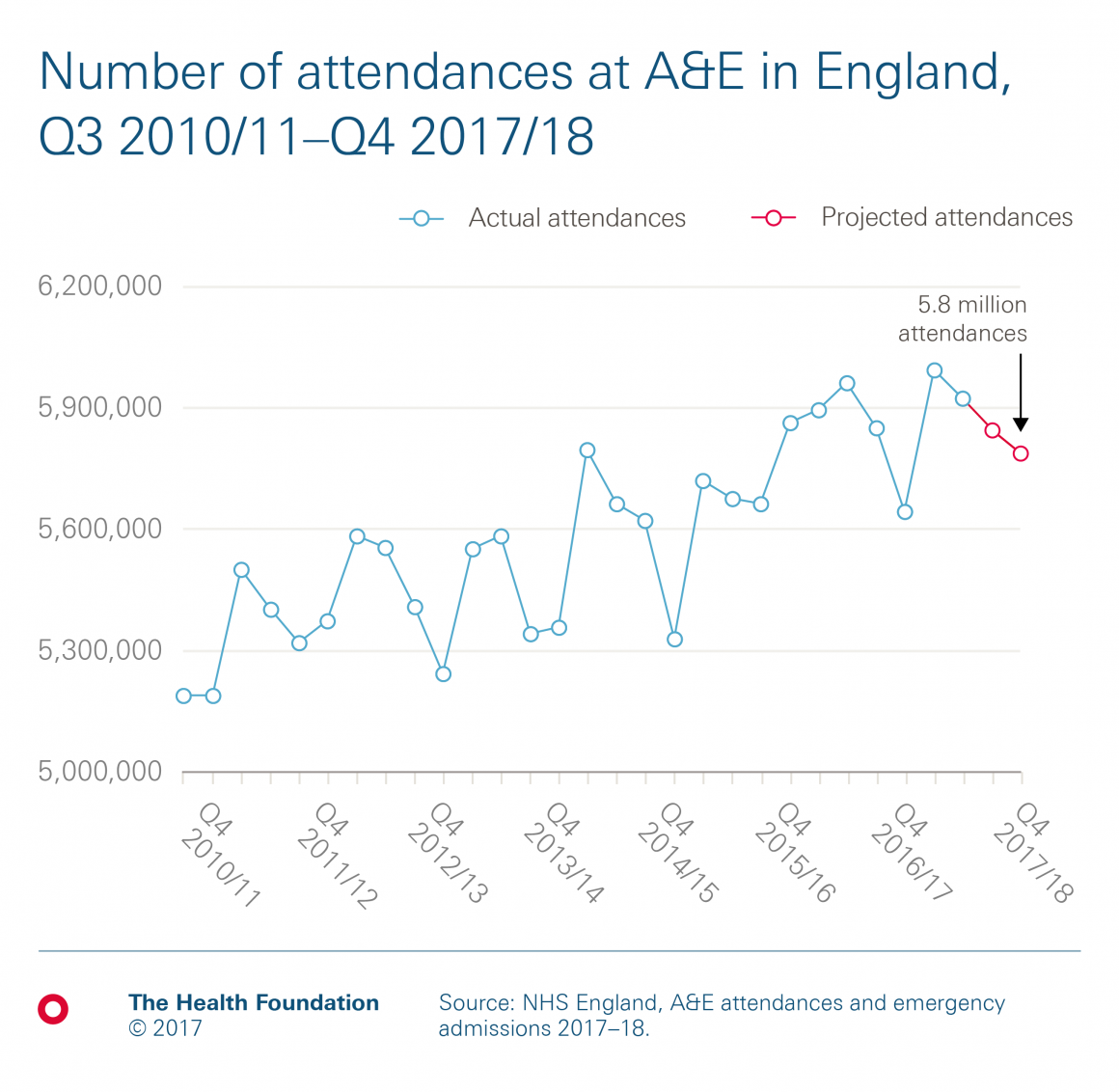
Chart 1: How many people are likely to attend A&E this winter?
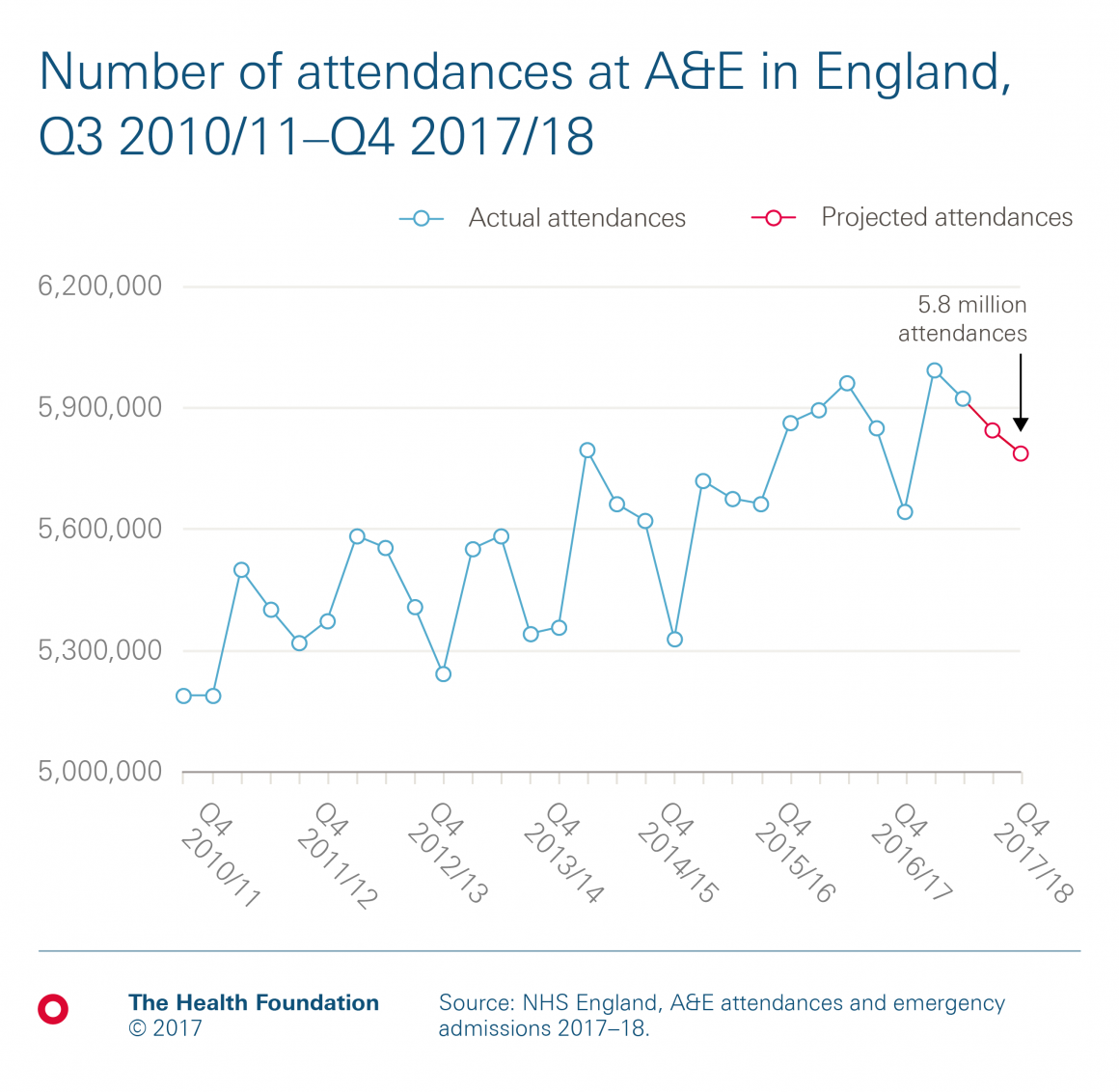
You will notice that there are actually fewer attendances at A&E in winter than at other times of the year. 5.9m people attended A&E in the latest quarter (July to September), and we actually project around 5.8m people to attend this winter (January to March). This is 600,000 more attendances than in winter 2010/11 (a 12% increase). However, the issue is not the number of people coming through the door. It is that more of the people who do come through the door take longer to treat, and are more likely to need to be admitted, adding pressure on available beds.
Chart 2: How many attendees are likely to wait longer than 4 hours?
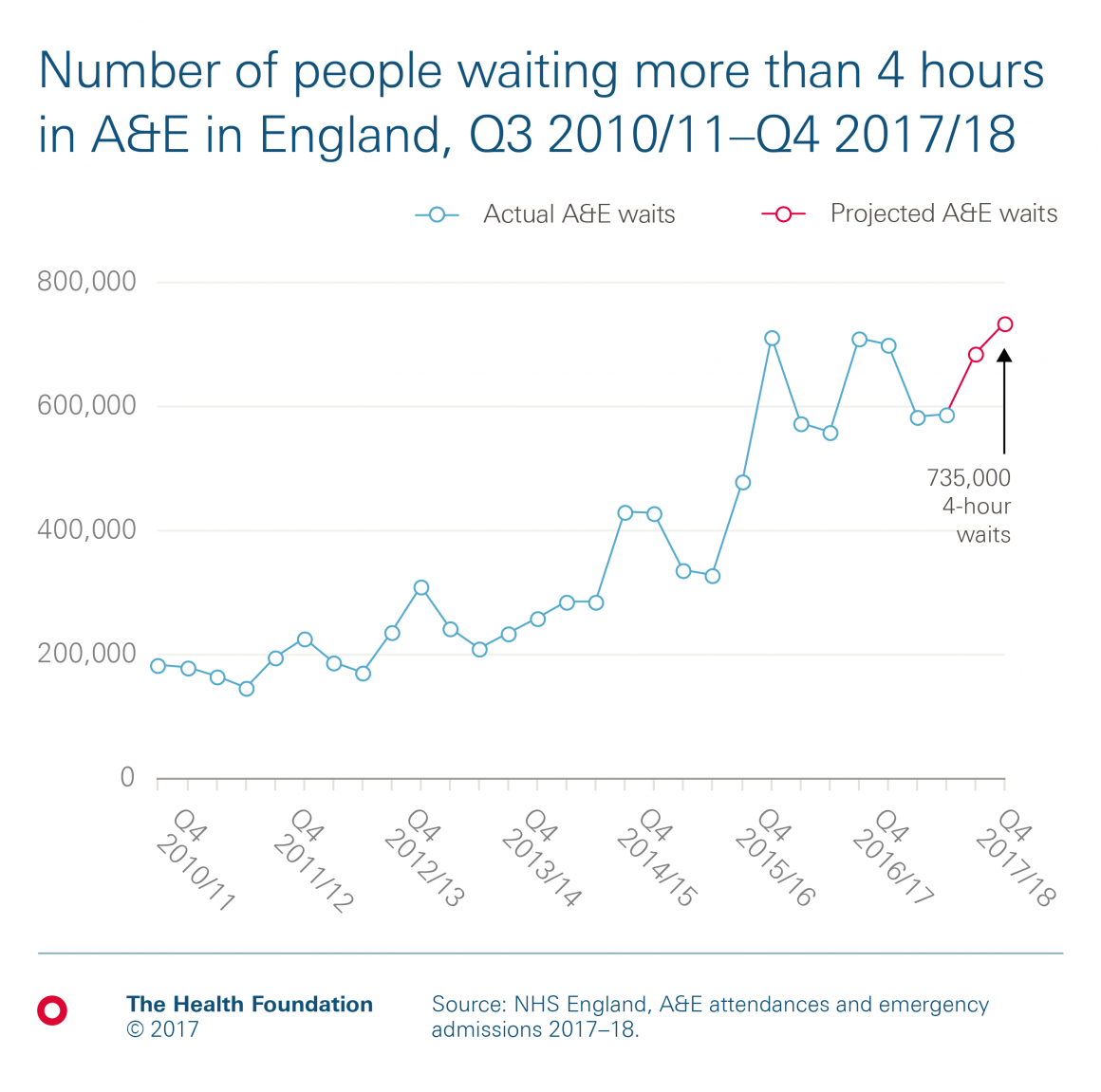
While the number of A&E attendances is lower in winter, more of them are severe enough to require an emergency admission. (We project around 1.1m admissions this winter, 19% of projected attendances). This means that the number waiting more than 4 hours is consistently higher. If this trend continues, our projections suggest around 735,000 people will wait longer than 4 hours in Q4 2017/18. That’s 150,000 more people than between July and September, and 311% higher than in the winter of 2010/11.
These projections together suggest that just 87% of people will be seen and treated within 4 hours in Q4 2017/18, which would potentially be the worst quarterly performance on record. Meeting the 95% target set in the mandate would require an additional 445,000 people to be seen and treated within 4 hours.
The average A&E attendance in 2015/16 cost £138. Cost inflation since then was estimated by NHS Improvement at 3.1% in 2016/17 and 2.1% in 2017/18, with an assumed efficiency growth of 2% each year. Using this, we have estimated a minimum cost of around £60m to help add capacity.
However, with lower numbers of attendances in winter, it’s not just about A&E capacity. The inpatient capacity needed to accommodate the additional admissions must also be addressed.
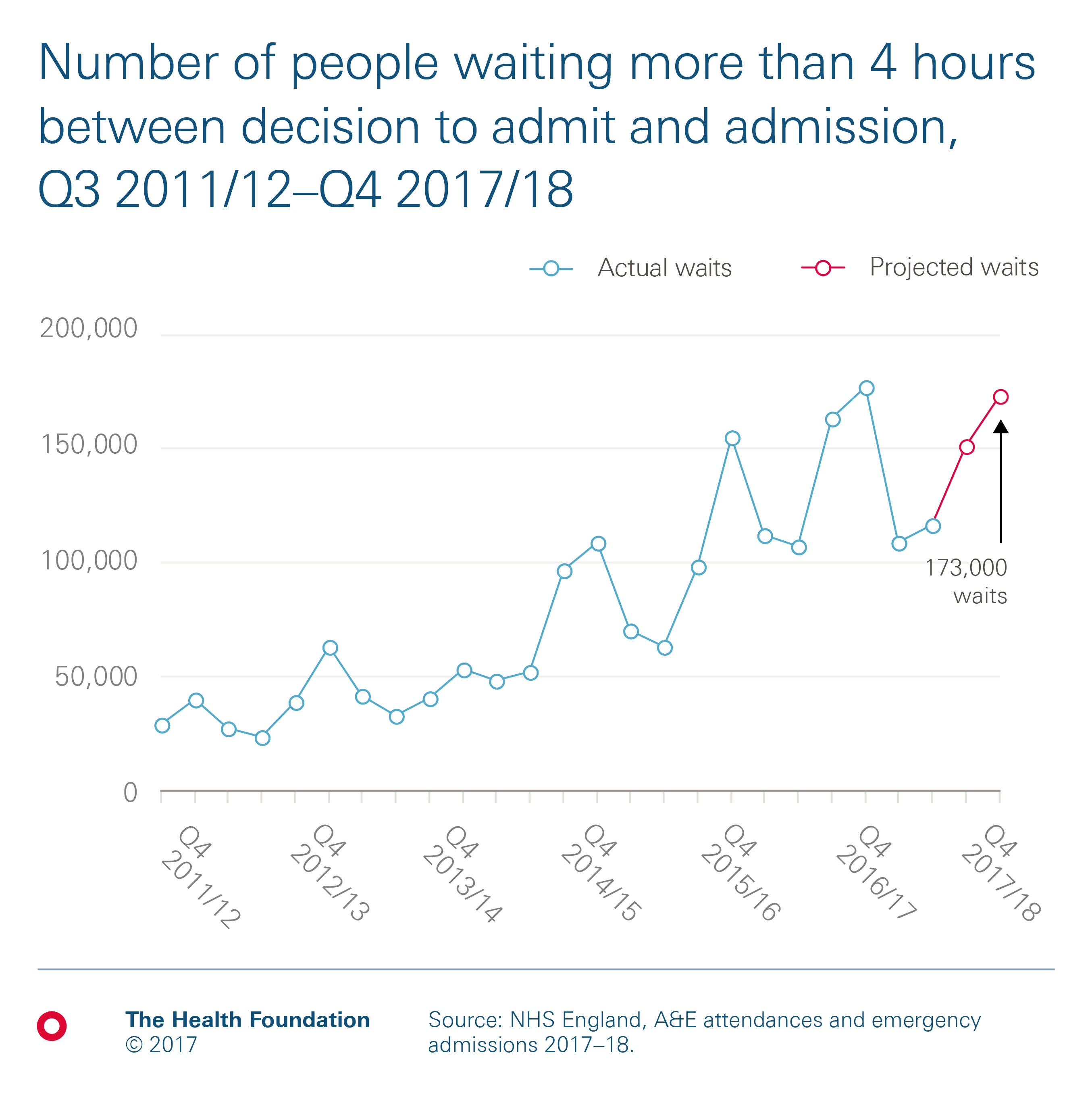
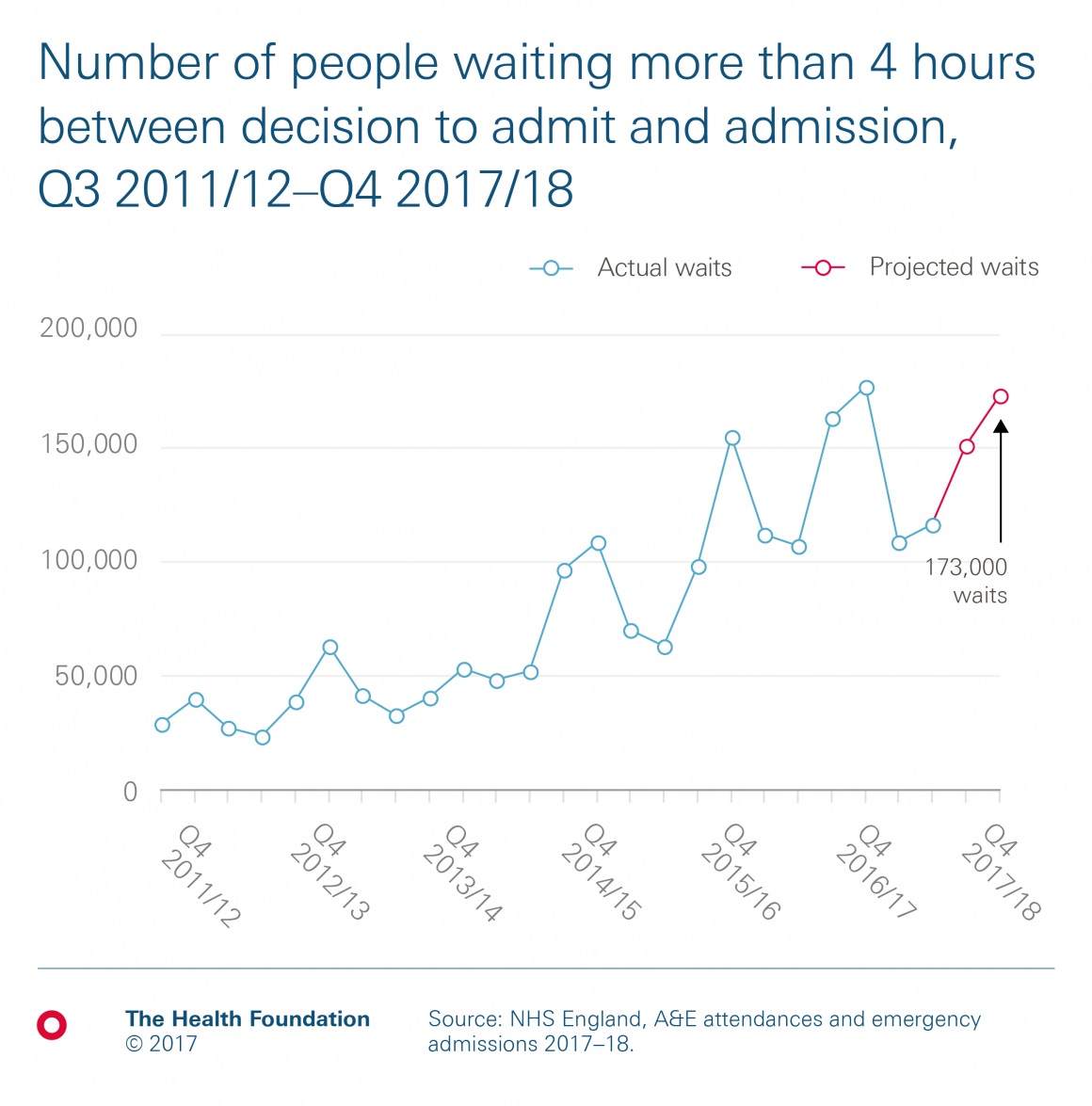
Chart 3: How many of these are severe enough to require an emergency admission to hospital, and wait longer than 4 hours to be admitted?
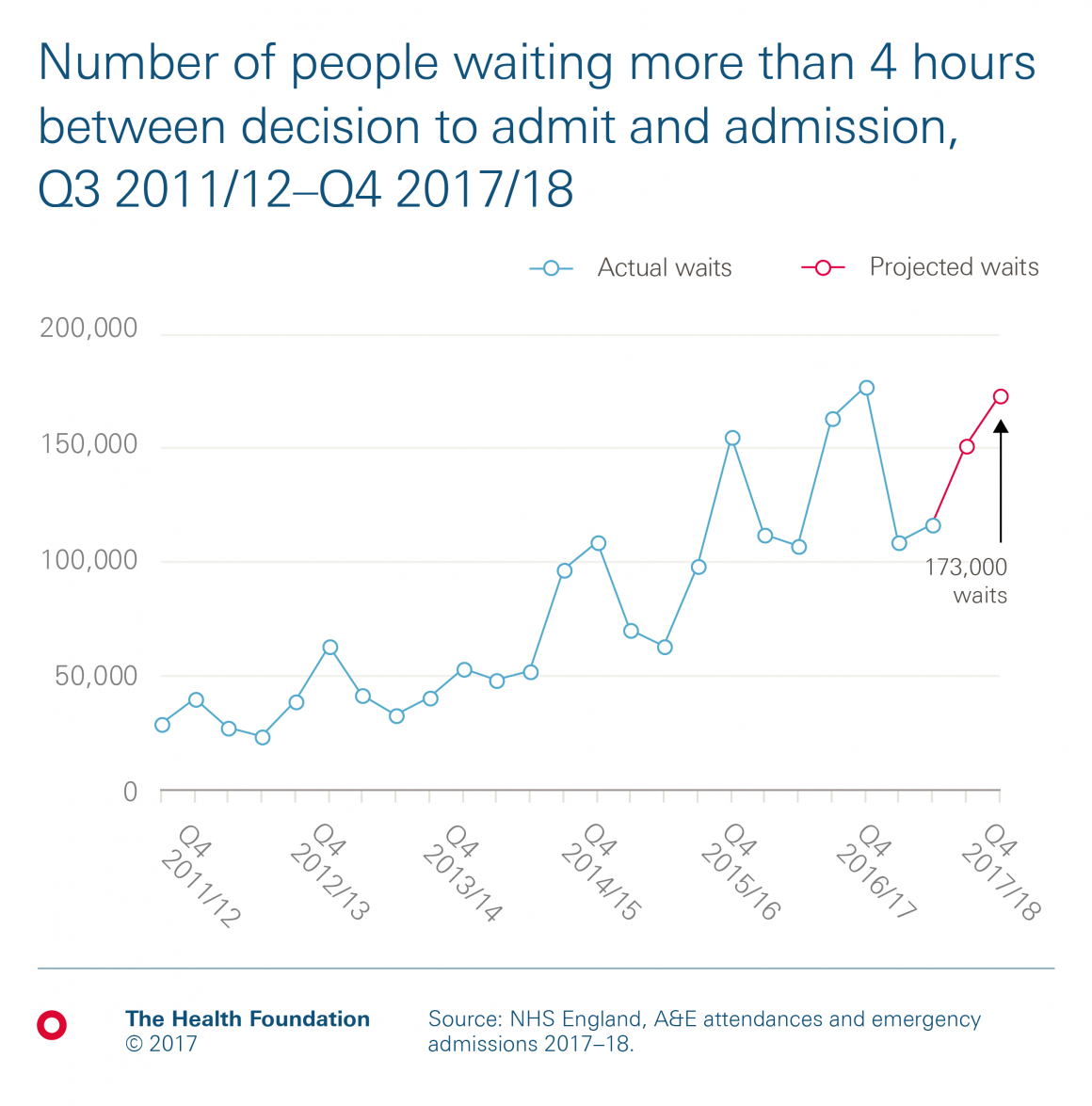
To estimate the additional capacity for admissions, we can look at the number of people who are waiting longer than 4 hours on a trolley. These are people who definitely need to be admitted, but for whom there isn’t a bed available yet, so they wait longer than 4 hours between the decision to admit and a bed being available. While this doesn’t account for all admissions over the 4-hour A&E target (which will be due to a combination of A&E capacity and bed availability), it provides a minimum estimate for the most severe cases. This group has grown by an average 40% a year since 2011/12, a total increase of 414% (albeit from a relatively low base). Again, you can see there’s a clear seasonal pattern. This winter, if this pattern continues, we would expect this to be around 173,000 people.
We estimate the average cost for an emergency admission from reference costs at just over £1,700. Applying the same adjustment for cost and efficiency as above, we estimate the extra cost of admitting this group of people would be around £300m.
So this gives our minimum estimate of £360m if we’re to increase both A&E and inpatient capacity to meet the 4-hour target this winter. This is similar to estimates from providers themselves.
How might the £360m be spent?
The more complicated question is how might this be spent. The first challenge is that it is not easy to predict where and when this additional capacity might be needed, so an oversupply of beds would almost certainly be required. The second is that there is already a shortage of nursing staff, so there would need to be a higher use of bank and agency staff to open these extra beds. This is a key cost area that NHS Improvement are trying to reduce. There is a similar argument for physical capacity. The cost of opening temporary beds or wards may be higher than maintaining current ones. This suggest that the true figure might be much higher.
The counterargument is that there has been £100m of capital investment to help ease winter pressures, more people have received the flu vaccine, and more 111 calls are handled by clinicians. If these measures are successful then the number of people waiting longer than 4 hours may buck the trend and be lower than we expect. Equally, we must acknowledge that people waiting are seen eventually, so the capacity does currently exist to treat them, but just not within the target time. Conversely the risk is that a major outbreak of flu or norovirus, or a severe drop in temperatures (which we have largely avoided in recent years), may buck the trend the other way.
This money might not be best spent in hospitals. Another way to increase hospital capacity is to reduce the number of delayed transfers of care (DTOCs), where people are medically fit to leave hospital but can’t due to delays arranging packages to support their return home. DTOCs were 65% higher in 2016/17 than in 2011/12. In Q4 2016/17, DTOCs accounted for 583,000 days, 5.2% of all hospital bed days.
Care packages to help people out of hospital are generally cheaper than treating them in acute care settings, so investing the money this way may be more effective. There is a target to reduce DTOCs to 3.5% of all hospital bed days. This target is backed by extra social care spending, announced in the last Budget, and would free up 215,000 bed days. But the drive to free up hospital capacity before winter has made only limited headway and, given how close we are to winter, achieving radical reductions in delays seems unlikely in the short-term.
With the temperatures already dropping, it is almost certainly too late to invest wisely in schemes to improve NHS performance this winter. But without at least some level of additional investment, it is hard to imagine how additional capacity can be found to improve access for patients who need emergency care this winter, next winter and beyond. Any additional investment would be welcome for this year, but a long-term plan needs to be developed as soon as possible for next year and those after. Winter is not going away.
Adam Roberts (@ADRoberts777) is Head of Economics at the Health Foundation
Further reading
Work with us
We look for talented and passionate individuals as everyone at the Health Foundation has an important role to play.
View current vacanciesThe Q community
Q is an initiative connecting people with improvement expertise across the UK.
Find out more

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}